
The short version
Semaglutide acts on one pathway (GLP-1). Tirzepatide acts on two (GLP-1 + GIP). Retatrutide acts on three (GLP-1 + GIP + glucagon). They are the first, second and third generations of the same family of peptides — not three brands of the same drug. Each generation adds a mechanism the previous one lacked. Retatrutide is the newest of the three and, as of 2026, still finishing its full trial programme.
If you have arrived at this page, you are probably weighing one peptide against the other two — not asking "what is a peptide". Good. This guide is written for that exact decision, in plain language, with the things hidden in marketing copy brought into the open.
What's in this guide
- Retatrutide, tirzepatide and semaglutide — same family, three generations
- Semaglutide — the original
- Tirzepatide — the dual-action successor
- Retatrutide — the triple-action newcomer
- The side-by-side comparison
- UK availability and legal status
- What each one actually costs in the UK
- Pen vs vial — the format question
- Which one fits which buyer
- Five mistakes UK buyers make
- FAQ
Retatrutide, tirzepatide and semaglutide — the same family, three generations
Semaglutide, tirzepatide and retatrutide are not three competing drugs in the way that, say, paracetamol and ibuprofen are. They are three consecutive generations of the same class of peptide. Each one was designed to act on more receptors than the last.
Reading them as a chronological line is the single most useful frame:
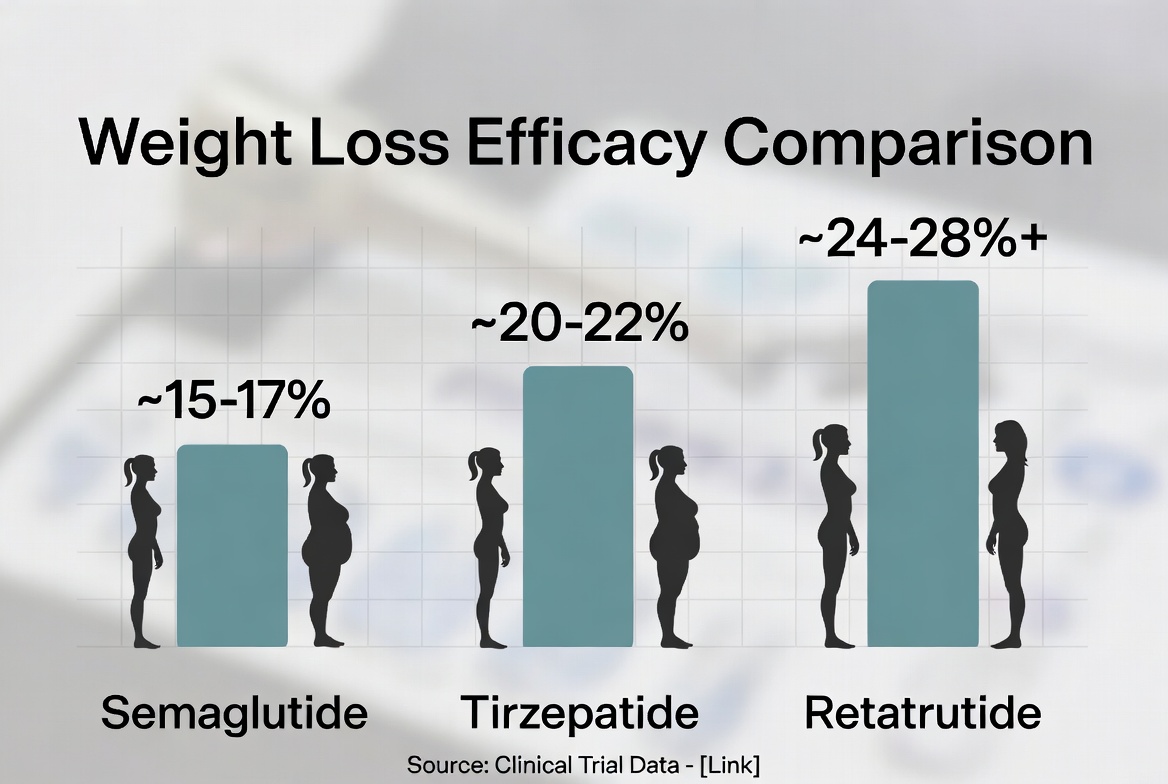
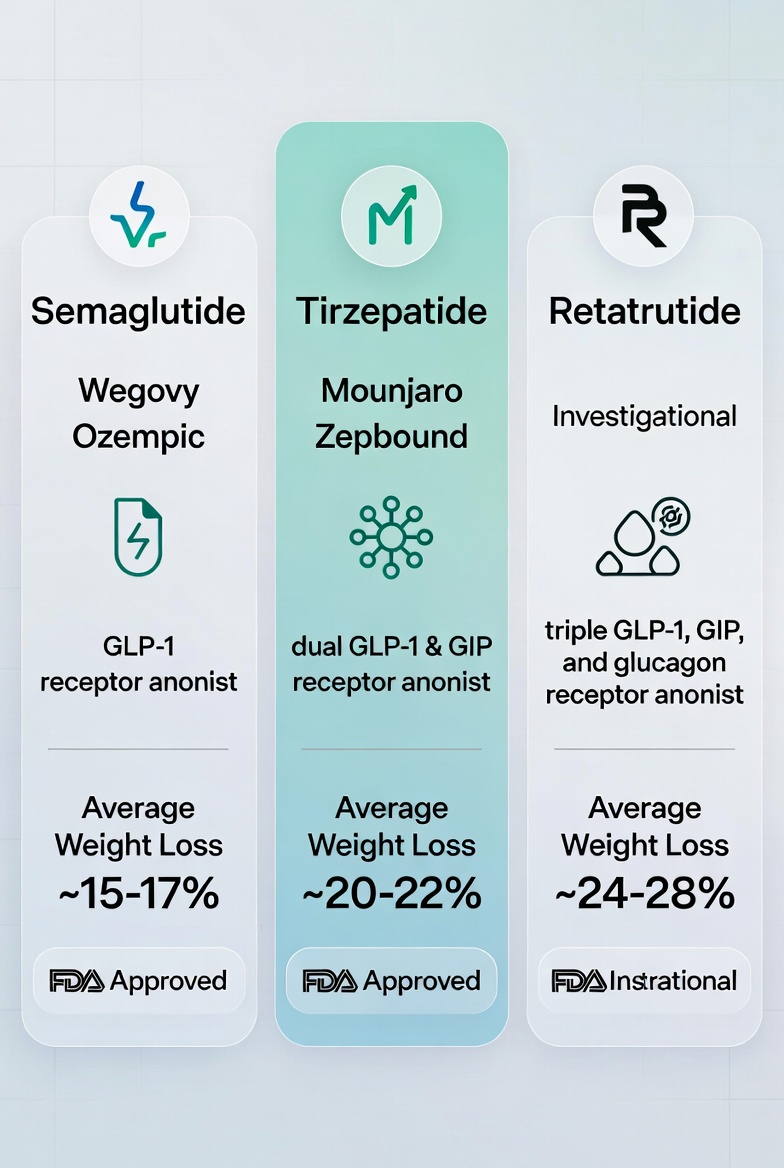
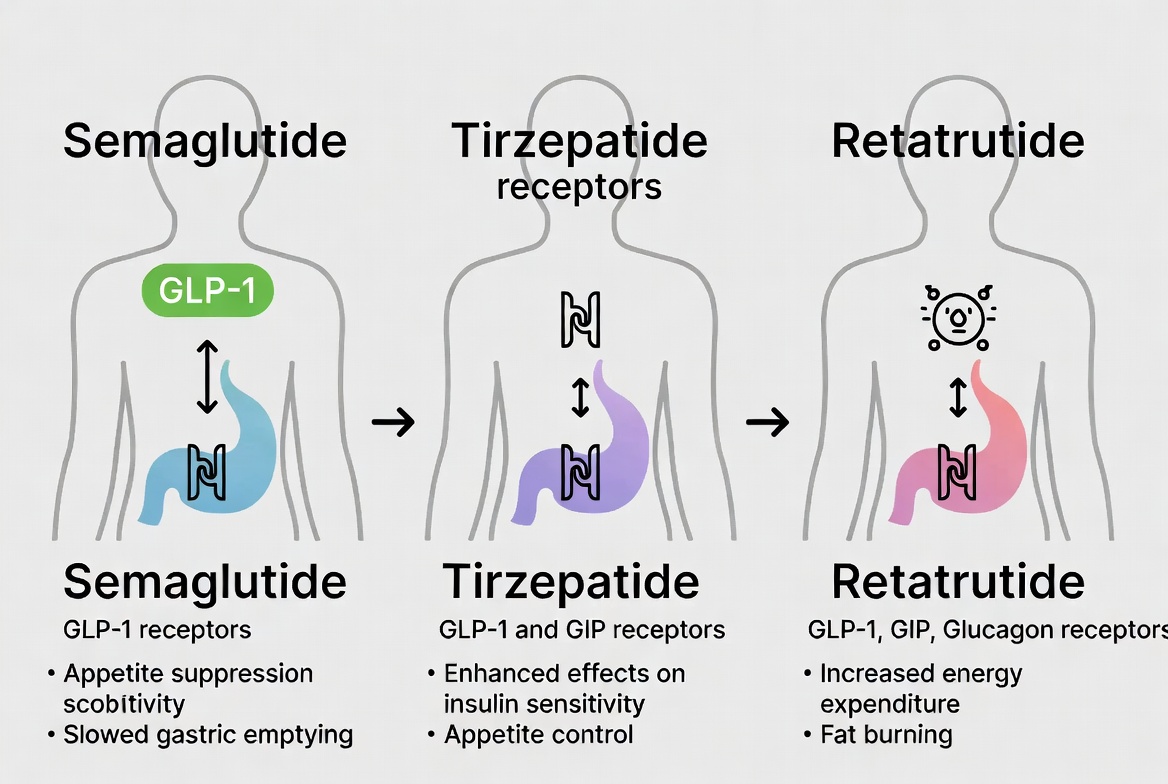
- Semaglutide is a GLP-1 receptor agonist. It mimics the gut hormone GLP-1, which influences blood-sugar regulation and satiety signalling.
- Tirzepatide is a dual GLP-1 / GIP receptor agonist. It adds the GIP pathway on top of GLP-1.
- Retatrutide is a triple GLP-1 / GIP / glucagon receptor agonist. It adds a third pathway — glucagon receptor activity — on top of the other two.
Each added pathway is not just a marketing point. The glucagon arm in retatrutide, for example, is the reason it behaves measurably differently from tirzepatide in early-phase trial data. Adding a receptor is not a small thing — it changes the metabolic profile of the molecule meaningfully.
Why this matters
When you read claims that "retatrutide is just a stronger semaglutide," that is not quite right. It is a different molecule with different receptor activity. "Newer generation" is closer to the truth than "stronger version".
Semaglutide — the original
Semaglutide is the peptide most UK readers will already know, even if not by that name. It is the active ingredient sold under licensed-medicine brand names in some markets and, since the late 2010s, has been the reference point for the entire GLP-1 category.
Its mechanism is the simplest of the three. By mimicking GLP-1, semaglutide slows gastric emptying, contributes to satiety signalling, and supports glucose regulation. Once-weekly dosing made it practical for self-administration at scale; the format is what turned a clinical molecule into a household word.
In the UK, semaglutide is the most established of the three. There is more long-term data, more clinician familiarity, and more peer-reviewed literature than for either of the newer generations. For a buyer whose priority is "the most studied option in this class," semaglutide is unambiguously that option.
Tirzepatide — the dual-action successor
Tirzepatide was designed to do everything semaglutide does, plus engage the GIP receptor at the same time. GIP is another gut hormone involved in glucose-dependent insulin release and fat metabolism. In practice, this means tirzepatide tends to produce larger weight-related outcomes than semaglutide at comparable dosing in head-to-head trial data, with the dual mechanism cited as the likely reason.
From a buyer's perspective, the two big things that changed with tirzepatide were the size of effect and the price point. Tirzepatide is broadly priced at a premium over semaglutide in private channels, reflecting that it is newer and that demand has consistently outstripped supply since launch.
Tirzepatide also remains a once-weekly peptide, with the same general subcutaneous administration as semaglutide. The handling experience is broadly similar.
Retatrutide — the triple-action newcomer
Retatrutide is the newest of the three. It adds the glucagon receptor to the mix, on top of GLP-1 and GIP. The hypothesis behind glucagon receptor activity in this context is that — in carefully designed peptide form — it can contribute to energy expenditure and fat-mass-specific outcomes, rather than simply suppressing appetite.
Early-phase trial data published from the retatrutide development programme has been the talking point of the entire peptide space for the last 18 months. The headline numbers from those early trials are larger than what tirzepatide showed at the equivalent stage. That is the reason retatrutide is being talked about as a meaningful step beyond the previous generation rather than a marginal one.
The honest caveat: as of 2026, retatrutide has not yet completed every phase of its trial programme, and full UK marketing authorisation as a licensed medicine has not been granted. It is, today, a wellness-product peptide in the UK private-pay market, sold by brands like Retapen40 as a premium wellness product for adults 18 and over. It is not on the NHS, not prescribed by GPs, and not a regulated medicine.
The two-sided framing
Retatrutide is the newest and most mechanistically interesting of the three; it is also the least long-term-studied. Both are true. A calm buyer holds both in mind at the same time.
The side-by-side comparison
| Semaglutide | Tirzepatide | Retatrutide | |
|---|---|---|---|
| Receptor targets | GLP-1 | GLP-1 + GIP | GLP-1 + GIP + glucagon |
| Generation | 1st | 2nd | 3rd |
| Dosing rhythm | Once weekly | Once weekly | Once weekly |
| UK licensed-medicine status | Yes, in specific indications | Yes, in specific indications | Not yet (as of 2026) |
| NHS availability | Restricted to specific criteria | Restricted to specific criteria | No |
| Private-pay availability | Widely available | Widely available; supply variable | Available via wellness brands |
| Length of available data | Longest | Medium | Shortest |
| Typical UK private-pay band | From ~£100–200/month | From ~£180–300/month | From ~£90–200/month* |
*With multi-month plans like the Reta Pen 40 12-Month Protocol bringing the effective monthly cost down significantly.
UK availability and legal status
This is where the three peptides differ most sharply for a UK buyer, and where the most confusion sits online. Strip it back to the basics:
Semaglutide
Held by licensed-medicine brands for specific indications in the UK. Available through private prescription channels and, within strict criteria, through the NHS. The widest installed base of any of the three.
Tirzepatide
Also held by a licensed-medicine brand in the UK, with specific approved indications. Private-pay availability has been strong since launch, though periods of supply tightness have happened repeatedly. NHS access is restricted to defined criteria.
Retatrutide
As of 2026, retatrutide has not been granted full UK marketing authorisation as a licensed medicine and is not on the NHS. It is sold by UK wellness brands — including Retapen40 — as a premium wellness product for adults aged 18 and over, with no prescription required. It is not intended to diagnose, treat, cure or prevent any disease.
What each one actually costs in the UK
Prices in this category move all the time, and the only sensible thing is to give bands rather than fixed numbers. The figures below reflect typical UK private-pay ranges as of mid-2026, not licensed-medicine list prices.
Semaglutide generally sits in the £100–200 per month band privately, depending on dose, supplier and pharmacy. As the longest-established of the three, supply tends to be the most stable.
Tirzepatide tends to land £180–300 per month privately, with the premium reflecting both the dual mechanism and demand pressure that has persisted since launch.
Retatrutide in pen form sits in a wider band depending on plan size. The Reta Pen 40 Starter is £189 for a single pen covering roughly two months, which is £94.50/month equivalent. The 12-Month Protocol works out at £116.33 per pen, or roughly £58 per month equivalent — the lowest effective per-month rate of any peptide in this comparison.
The pricing reality
On a strict per-month basis, retatrutide via a multi-pen UK plan can be the most cost-efficient of the three. On a single-purchase basis, semaglutide tends to be the lowest entry-point. Tirzepatide is consistently the most expensive of the three in the UK private market.
Pen vs vial — the format question
The peptide is half the decision. The format you take it in is the other half — and this gets less attention than it deserves.
The pen format — a sealed cartridge inside a pre-loaded auto-injector that dials a precise dose at the click of a ring — has become the default for self-administration. It removes three of the most common friction points of older methods: manual measuring, the contamination risk of an open vial, and the awkwardness of laboratory glassware. For most UK buyers, this is the format worth defaulting to.
The vial-and-syringe format still exists, particularly in research-grade markets, and is sometimes cheaper per unit. It involves drawing each dose manually with a separate syringe, which adds steps, room for measuring error, and a higher contamination surface. The cost advantage usually does not survive the inconvenience for an ordinary buyer.
Retatrutide is increasingly available in the pen format in the UK — the Reta Pen 40 being a UK-finished example — which puts it in line with how semaglutide and tirzepatide have always been delivered in their licensed forms. If you have used a pen before, the handling will feel familiar.
